The Alternative Treatments
Hysterectomy
Although the first hysterectomy was performed in 1483, the majority of patients who had this procedure died, mainly from sepsis, and it was only with the introduction of anaesthesia, antibiotics and aseptic techniques that hysterectomy began to become a safer procedure.
It involved the removal of the uterus containing the fibroids and usually the cervix.
However hysterectomy is a major surgical procedure carrying a serious complication rate of around 4-6% and a death rate of approximately 1-1500; approximately 30,000 hysterectomies for fibroids are carried out in the UK alone.
There is a long list of possible complications from hysterectomy which include:
- Piercing of bowel, bladder and ureter with further major surgery
- Pelvic abcess
- haemorrhage
- adhesions
- keloid scarring
- deep venous thrombosis
- Pulmonary embolus which may be fatal
- Delayed bowel obstruction
- Vaginal prolapse
- Possible weakening of the pelvic floor? with effect on bladder and bowel function
A lot of the complications require another major surgical operation.
In recent years, many alternative treatments for fibroids have been devised.
Myomectomy
The usual surgical alternative to hysterectomy is abdominal myomectomy. In the latter procedure the surgeon attempts to cut out the fibroids leaving the normal part of the womb intact. Myomectomy has been used widely for decades but it is a difficult operation with a significant complication rate. In addition, importantly, there is a high recurrence rate of >70% (Hanafi et al 2005) that occurs in patients with multiple fibroids. A high percentage of patients having myomectomies will require re-operation for recurrence usually hysterectomy. In fact figures show 20% of women will have had hysterectomies within 5 years of myomectomy (Reed et al, 2006).
Laparoscopic (keyhole surgery) myomectomy is an effective, much less invasive, procedure but there are major limitations on the size and number of fibroids that can be treated. Again this surgery has a higher complication rate than UAE
Open myomectomy and laparoscopic myomectomy comlications include:
- Piercing of bowel, bladder and ureter with further major surgery
- Pelvic abcess
- Haemmorhage
- Adhesions which may lead to bowel obstruction
- Morcellation of uterine sarcoma
- Port herniation
- Keloid scarring
- Deep venous thrombosis
- Pulmonary embolus which may be fatal
- 0.5% to 1% hysterectomy rate
- Failed or partially completed procedures
- High recurrence rate
- Uterine rupture, particularly intra partum
- Neuropathy
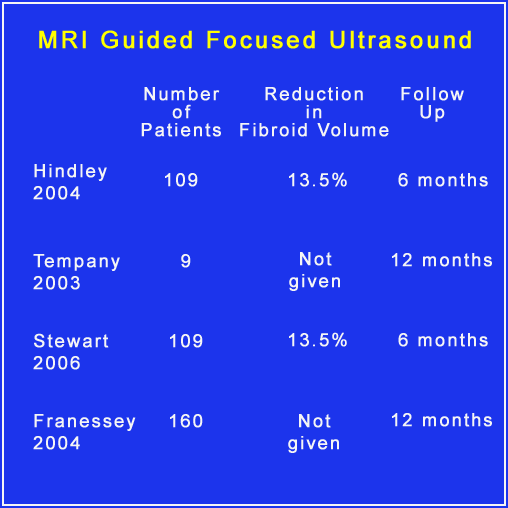
MRI Guided Ablation
Another technique for treating fibroids is MRI guided ablation either laser ablation or ultrasound ablation. Essentially under the control of MRI fibroids are subjected to intense internal heating which kills off the heated tissue. The problem with the procedure is that it quite often only destroys part of the fibroid leaving viable tissue which grows and is only indicated for certain fibroids in certain positions. In addition, although the procedure has been available for at least two decades significant long term studies have not been published. Shrinkages in published papers with relatively short follow ups have been low.
Fibroid embolisation of course in contrast can be used to treat single or multiple fibroids has the advantage of killing all the fibroids at one session with only a minimal recurrence rate.
Medical Treatment
The usual medical treatment is to give patients a drug called a GNRH analogue (gonadotrophin releasing hormone analogue) which affects the release of hormones from the pituitary gland and produces an artificial menopause: Zoladex would be a typical example. The problem is these drugs are only effective in less than 50% of women and they may have unpleasant menopausal side effects and have to be stopped after 3 or 4 months or they can cause more problems. When the GNRH treatment is stopped, the fibroids tend to grow back very quickly. Thus these days when there are alternatives to major surgery procedures like hysterectomy, it is dubious whether GNRH analogues are indicated in the treatment of patients with severe fibroid symptoms unless there is a really good reason for a temporising measure.
Another problem with GNRH analogues is if they are given a definitive treatment like fibroid embolisation it has to be delayed for 3 months following the last injection. In patients wishing to become pregnant who have fibroids, patients are usually offered a myomectomy.